 |
| Image from https://www.emaze.com/@ALRRWOTC |
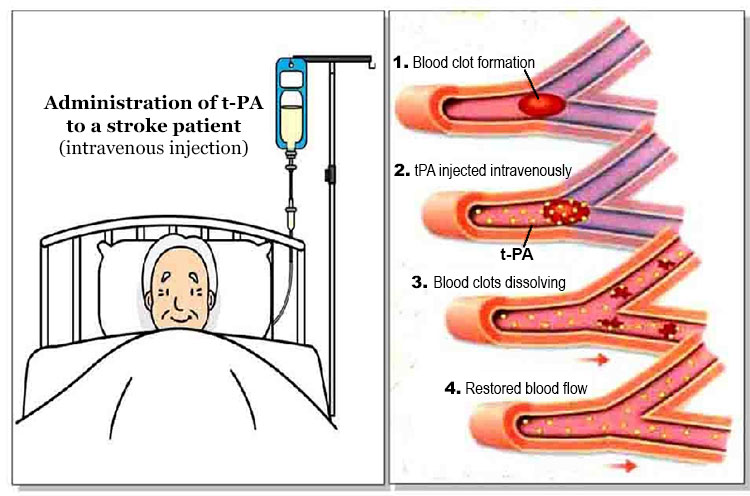
Here is a very brief run down on thrombolysis:

1) Time is brain
The most important thing to know about this treatment is that "time is brain", there is a ticking clock that starts from the moment that you've had the stroke. You only have 4.5 hours to get to the hospital, have a CT scan to exclude bleeding in the brain and start the process. This is why it is important to know the signs of a stroke and act quickly. Thrombolysis comes with a small yet significant chance of having a bleed in the brain. Once you pass the 4.5 hour mark the risks start to outweigh the benefits.
2) Things happen quickly
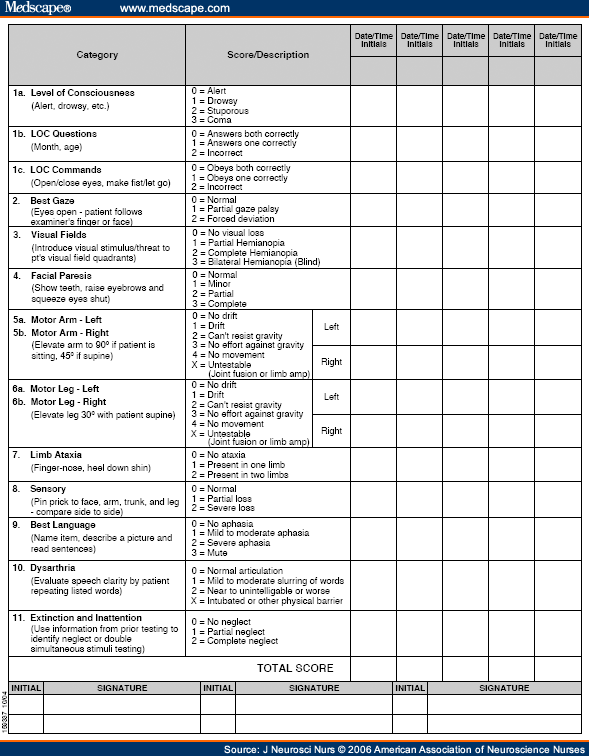
I've met a patient who said no to thrombolysis for two reasons, the first was they were not entirely convinced that they had the onset time of the stroke correct, and the second was because they had to make the decision so quickly they saying no seemed like the best option at the time. They'd already had a minor stroke, why risk an additional bleed on the brain? His doctors were a bit salty about this decision, from the patients reports anyway. I understand both the patient and the doctor (if they were indeed a bit frustrated). Some people just don't like making decisions quickly. But also we have the cool up and coming procedure, let it work for you too! So what happens quickly? They do a CT, complete a set of bloods, complete a medical history to ensure no contraindications and they complete the NIHSS (see below) and if you score within a certain range you're eligible.
I've met a patient who said no to thrombolysis for two reasons, the first was they were not entirely convinced that they had the onset time of the stroke correct, and the second was because they had to make the decision so quickly they saying no seemed like the best option at the time. They'd already had a minor stroke, why risk an additional bleed on the brain? His doctors were a bit salty about this decision, from the patients reports anyway. I understand both the patient and the doctor (if they were indeed a bit frustrated). Some people just don't like making decisions quickly. But also we have the cool up and coming procedure, let it work for you too! So what happens quickly? They do a CT, complete a set of bloods, complete a medical history to ensure no contraindications and they complete the NIHSS (see below) and if you score within a certain range you're eligible.
 |
| https://www.medscape.com/viewarticle/550818_2 NIHSS |
3) How to be included.
I think that the inclusion/exclusion criteria will change with time and further research. Right now to be included, besides getting a goldilocks NIHSS score, and a CT that shows no bleeding or trauma. You need to be over the age of 18 and under the age of 80*. Not pregnant*. Not had the stroke in your sleep or a Wake Up Stroke (WUS)*. Your BP need to be under control. No previous strokes in the past three months. No use of heparin in the last 48 hours.
For all of the * criteria, I am seeing literature emerge that is saying that these shouldn't be automatic exclusions, there are a few authors arguing for a less black and white approach to identifying who is eligible. A "case by case" approach, if you will.
4) Would I consent?
I've read the word small yet significant chance of haemorrhage so many times that I think that it's lost all meaning. I've read so many studies about the amazing functional gains that I don't think I would hesitate in consenting for me or any of my loved ones who've given me EPOA. Yes, I would.


No comments:
Post a Comment